
Shoulder pain |
shoulderpaintreatment
@Physio4athletes
Have you injured your shoulder?
We have treated people of all ages and capabilities with shoulder pain, who do many different activities including the list below:
Swimming (competitive, masters, recreational, open water, paralympians & olympians); Tennis; Water polo; Baseball; Cricket players, Basketball & wheelchair basketball; Netball; Circus athletes; Jockeys; Track cyclists; Gardeners; Craft enthusiasts; Domestic workers; Tradespeople- carpenters, electricians, plumbers, labourers; Cleaners; Delivery personnel; Hospitality workers; Health care workers (nurses, GP, surgeons) ; Beauticians; Hair dressers; Boxers; Gym enthusiasts; Weight lifters, Footballers, Cricketers, Dancers, Yoga, Rock climbers.
We are certain we have missed some, but the message is no matter what you want to do with your shoulder, or how old you are, we are here to assist you.
We have treated people of all ages and capabilities with shoulder pain, who do many different activities including the list below:
Swimming (competitive, masters, recreational, open water, paralympians & olympians); Tennis; Water polo; Baseball; Cricket players, Basketball & wheelchair basketball; Netball; Circus athletes; Jockeys; Track cyclists; Gardeners; Craft enthusiasts; Domestic workers; Tradespeople- carpenters, electricians, plumbers, labourers; Cleaners; Delivery personnel; Hospitality workers; Health care workers (nurses, GP, surgeons) ; Beauticians; Hair dressers; Boxers; Gym enthusiasts; Weight lifters, Footballers, Cricketers, Dancers, Yoga, Rock climbers.
We are certain we have missed some, but the message is no matter what you want to do with your shoulder, or how old you are, we are here to assist you.
About Shoulder pain
Shoulder pain is one of the most common musculoskeletal complaints treated in physiotherapy clinics throughout Australia. Certainly at Physio4athletes we see many clients each year with shoulder pain ranging from a minor 'niggle' to severe pain that is affecting many aspects of daily life, self care and exercise. Shoulder pain commonly presents in the "sub acromial" area, but can also radiate towards the neck, behind the shoulder or down the arm. Your physiotherapist will assess whether there is any contribution from your neck to your shoulder pain (referred pain).
Basic shoulder anatomy
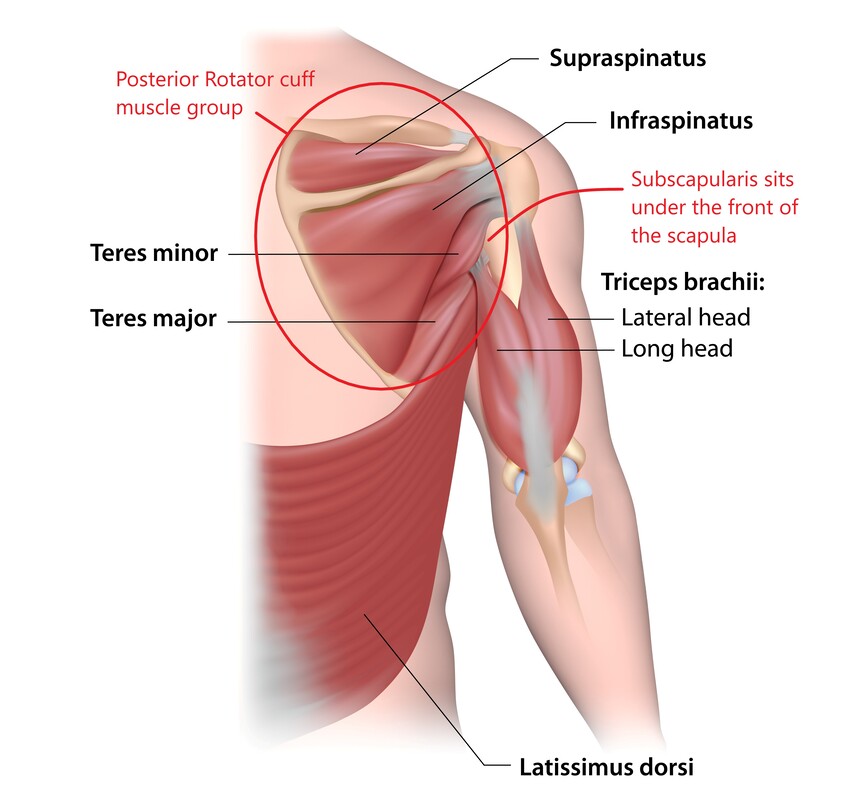
There are a number of structures located in the shoulder area that can generate pain and these include the rotator cuff tendons, acromioclavicular joint (AC joint), bursa, biceps tendon, labrum and joint capsule and ligaments (Figures 1 & 2).

We have found that understanding the functional anatomy of the shoulder is helpful for patients. The "shoulder complex" has 3 bones, being the humerus (arm bone), scapula (shoulder blade) and clavicle (collar bone). There is a joint between the collarbone and the shoulder blade (AC joint) and between the scapula and humerus (glenohumeral joint) as shown in Figure 1. The glenohumeral joint is a ball and socket joint, with the socket or base being on the scapula and the ball part on the end of the arm bone (Figure 1). This joint is the most mobile in the body and allows us to move our arms in many directions. The shoulder has ligaments and labrum (cartilage) which work together with the muscles to stabilise the joint during movement. The ball and socket joint allows for arm motion up, down, backwards, sideways and rotation, along with many combinations of these movements. This arm movement is assisted by motion of the scapula (shoulder blade) on the rib cage. We often don't notice that we can shrug, pull back, tilt and rotate our shoulder blades and that this changes the positioning of the socket of the shoulder joint.

Movement of the shoulder is generated by "prime mover" muscles such as the Deltoid, Latissimus Dorsi (lats) and pectoralis major and minor (pecs). The rotator cuff muscle group (Figure 2) provide essential control of movement of the ball in the socket and these tendons are commonly injured. The scapula stabilising muscles - trapezius, rhomboids and serratus anterior play an important role as they position the shoulder blade during arm motion. Precise co-ordination of muscle activity and good strength is required for optimal full shoulder function making this joint a great candidate for well-planned exercise therapy.
Injury causationEach patient's "injury story" is very important to the clinical picture, diagnosis and rehabilitation plan. Where shoulder pain is a result of a distinct injury such as a fall, a tackle during sport or awkward lift overhead, imaging and clinical tests are sometimes used to assist with identifying a specific structural injury.
A note on imaging - the results should be considered in context with the individual's clinical picture as many scans show findings that are not related to symptoms. The old adage "treat the patient not the scan" is relevant here. When shoulder pain arises and there has not been a "traumatic injury", careful questioning usually identifies triggers for the pain, such as a recent change in use of the shoulder. More likely than not, the individual has performed activities that exceeded their shoulder's current 'load capacity' or amount of work/effort that their shoulder can comfortably manage. Some clinical examples of this that we have seen are: - Increasing rapidly the amount of sprint swimming performed at training - Suddenly working more in the garden doing heavy digging - Quickly increasing overhead lifts or pull ups in gym - Returning to tennis after a 6 month break - Resuming throwing at the beginning of a cricket season - Starting shoulder side stands in Yoga class At times, shoulder pain is "idiopathic" in origin, which means symptoms are spontaneous and of unknown cause- an example of this is frozen shoulder (adhesive capsulitis). Another distinct shoulder problem is multi-directional instability, where, in the absence of any trauma, the shoulder joint dislocates or subluxes (slips out of place) frequently, in more than one direction, during an individual's normal activities. |
Common shoulder complaints- Rotator cuff related shoulder pain- tendinopathy, partial or full thickness tendon tears, usually involving supraspinatus, then infraspinatus and less frequently subscapularis.
- Bursitis, usually associated with a tendinopathy - Biceps tendinopathy and tendon tears - AC joint pain (acromioclavicular joint) - Subacromial pain syndrome (this is another name for rotator cuff and bursitis problems) Less common: - Labral tears - Shoulder instability: traumatic or non traumatic - Capsulitis - Other: glenohumeral joint osteoarthritis, calcific tendonitis Beyond "Shoulder impingement"
Historically, shoulder impingement was described by Neer in 1972 as a theory for the development of rotator cuff tendon injuries (1). "Shoulder impingement" theory proposes that as the arm is raised, the bony acromion makes contact with and pinches or 'impinges' the underlying rotator cuff tendons and bursa, causing painful movement and, presumably, tendon damage over time. For the next 4 decades this was the dominant theory for why rotator cuff pain developed and guided treatments including decompression surgery (acromioplasty). More recently, it is understood that rotator cuff tendons develop an overuse tendinopathy similar to other tendons in the body and essentially show a failed healing response after excessive or repetitive loading. Contact between the tendons/bursa and bone is a normal physiological occurrence(2). With respect to treatment, there is emerging evidence that physiotherapy directed exercise therapy is the preferred approach for patients with this presentation (3,4). |
Shoulder pain treatment

At Physio4athletes, we have a long history of treating people who ask a lot of their shoulders during their
sporting pursuits and daily life. Our shoulder pain treatment is INDIVIDUALISED according to your injury (5)
but is broadly divided into 3 phases that we call:
1. Acute
2. Build
3. Consolidation
Physiotherapy management includes a combination of passive (hands on techniques) and active treatments (exercises that you perform) (3,4). Rehabilitation results are improved when all phases of treatment are completed and exercises are continued, rather than stopping as soon as the pain settles and function returns.
sporting pursuits and daily life. Our shoulder pain treatment is INDIVIDUALISED according to your injury (5)
but is broadly divided into 3 phases that we call:
1. Acute
2. Build
3. Consolidation
Physiotherapy management includes a combination of passive (hands on techniques) and active treatments (exercises that you perform) (3,4). Rehabilitation results are improved when all phases of treatment are completed and exercises are continued, rather than stopping as soon as the pain settles and function returns.
1. ACUTE PHASE
GOAL: Pain modulation, regain mobility, introduce safe strengthening exercises & modify training/activity levels to allow for symptom reduction
TREATMENTS: Manual therapy, taping, dry needling (where indicated), home icing (4), isometric & low range shoulder exercises (4), stretches.
GOAL: Pain modulation, regain mobility, introduce safe strengthening exercises & modify training/activity levels to allow for symptom reduction
TREATMENTS: Manual therapy, taping, dry needling (where indicated), home icing (4), isometric & low range shoulder exercises (4), stretches.


2. BUILD PHASE
GOAL: Develop shoulder strength. Gradually build up training and activity
TREATMENTS: Manual therapy, progressive strength exercises for rotator cuff, scapular & prime mover muscles. Re-loading plan, sports technique correction if required.
STRENGTH TESTING: Dynamometry can be used to identify weaknesses and target exercises
GOAL: Develop shoulder strength. Gradually build up training and activity
TREATMENTS: Manual therapy, progressive strength exercises for rotator cuff, scapular & prime mover muscles. Re-loading plan, sports technique correction if required.
STRENGTH TESTING: Dynamometry can be used to identify weaknesses and target exercises



3. CONSOLIDATION PHASE
GOAL: Continue to build strength to improve the shoulder's overall tolerance to load whilst doing full training/activity
TREATMENTS: Increase the complexity and challenge of strength and exercises
Strength testing to detect any changes and track progress
GOAL: Continue to build strength to improve the shoulder's overall tolerance to load whilst doing full training/activity
TREATMENTS: Increase the complexity and challenge of strength and exercises
Strength testing to detect any changes and track progress



References:
(1) Neer CS, 2nd. Anterior acromioplasty for the chronic impingement syndrome in the shoulder: a preliminary report. J Bone Joint Surg Am. 1972;54(1):41-50.
(2) McFarland, Maffulli, Del Buono, Murrell, Petersen; Impingement is not impingement: the case for calling it “Rotator Cuff Disease”; Muscles Ligaments Tendons J, 2013 Jul-Sep; 3(3): 196–200.2013 Jul-Sep; 3(3): 196–200.
(3) Nazari et al, The effectiveness of surgical vs conservative interventions on pain and function in patients with shoulder impingement syndrome. A systematic review and meta-analysis, PLoS, 2019:; 14 (5)
(4)Steuri et al, Effectiveness of conservative interventions including exercise, manual therapy and medical management in adults with shoulder impingement: a systematic review and meta-analysis of RCTs, British Journal of Sports Medicine, Vol 15 (18).
(4) Dupuis F, et al. Cryotherapy or gradual reloading exercises in acute presentations of rotator cuff tendinopathy: a randomised controlled trial BMJ Open Sport Exerc Med 2018;4:e000477. doi:10.1136/bmjsem-2018-000477
(5) Lewis J et al Rotator Cuff Tendinopathy: Navigating the Diagnosis-Management Conundrum, JOSPT 2015 14:11.
(1) Neer CS, 2nd. Anterior acromioplasty for the chronic impingement syndrome in the shoulder: a preliminary report. J Bone Joint Surg Am. 1972;54(1):41-50.
(2) McFarland, Maffulli, Del Buono, Murrell, Petersen; Impingement is not impingement: the case for calling it “Rotator Cuff Disease”; Muscles Ligaments Tendons J, 2013 Jul-Sep; 3(3): 196–200.2013 Jul-Sep; 3(3): 196–200.
(3) Nazari et al, The effectiveness of surgical vs conservative interventions on pain and function in patients with shoulder impingement syndrome. A systematic review and meta-analysis, PLoS, 2019:; 14 (5)
(4)Steuri et al, Effectiveness of conservative interventions including exercise, manual therapy and medical management in adults with shoulder impingement: a systematic review and meta-analysis of RCTs, British Journal of Sports Medicine, Vol 15 (18).
(4) Dupuis F, et al. Cryotherapy or gradual reloading exercises in acute presentations of rotator cuff tendinopathy: a randomised controlled trial BMJ Open Sport Exerc Med 2018;4:e000477. doi:10.1136/bmjsem-2018-000477
(5) Lewis J et al Rotator Cuff Tendinopathy: Navigating the Diagnosis-Management Conundrum, JOSPT 2015 14:11.